
Capacity planning: feed-the-beast, or vital management information?
24/09/2014by Rob Findlay
On the 16th September I had the privilege of speaking to the Association of Professional Healthcare Analysts at their conference in Bristol. This is a lightly edited version:
I’d like to start with a couple of questions for you:
The first question is: How many of you, in your NHS careers, have ever run the numbers for a business case – for a consultant appointment or capital scheme? [quite a few hands went up] Now keep your hands up if you felt that your analysis was usually reflected in real-world change. [about two-thirds kept their hands up]
Second question: hands up if you have ever run the numbers for the annual contracting and planning round? [a larger number of hands went up] Now keep your hands up if you felt that your analysis was usually reflected in real-world changes as a result. [nobody kept their hands up]
Interesting. The thing is, everybody agrees that planning is a Good Thing. So in the NHS we do a lot of it.
We have business cases; 5 year strategic plans; 2 year operating plans; annual contracting plans; backlog clearance plans; system resilience plans, plans for year-end, quarter-end and month-end; plans for winter, spring, summer and autumn; and now we have plans for the run-up to the General Election.
The very long range plans for business cases work pretty well. They are carefully constructed, demand based, and capacity really does change in line with demand as a result of them.
But what about these annual plans, that are drawn up every winter between providers and commissioners? The little poll we did just now suggests these plans don’t change real life very much. Why is annual planning less ‘real’?
Well, let’s look at the process.
The annual planning process
Any genuine planning has to involve the operational managers who are going to deliver it. So Step 1 for the annual planning round is to carefully engage them and ask them to help develop plans for their part of the service. This immediately runs the risk of cobbling together lots of little plans, each of them based on different methods, assumptions, and data sources.
Step 2 is when we add all those plans together, and find out we don’t have a big enough hospital or quite enough money to deliver them.
Step 3 is the effort to bridge the gap, and this involves commissioners as well as hospitals. Here there can be confusion even about fairly straightforward things, so you might hear commissioning managers saying things like: “but that can’t be your demand: we didn’t buy that much”.
As analysts, you know the distinction between activity, capacity and demand: activity is the work you do; capacity is the work you could do; and demand is the work you need to do to avoid falling behind. But it is surprising how often those things are confused.
Step 4 is the final rush to sign off the contract. The gap has to be bridged somehow, so here we might get some brave assumptions about demand management and shifts into primary care, some benchmarked performance assumptions, a slice taken out of the non-tariff spend, and a 5% CRES at the hospital end.
And so the process comes to a successful end, in the sense that a document was signed off.
Actually, not quite the end. There is a Step 5. That comes several months later when the Trust goes back to the CCG for the contingency fund. Everyone knows that commissioners tuck a few million away in their back pocket just in case. A few years ago at one of these mid-year meetings I was delighted to hear an operational manager complain: “I’ve got hips coming out of my ears”.
The game here is to pretend this is non-recurring funding, to cover a one-off backlog clearance. This year even the government is joining in the fun, with the Elective Care Fund. And so with a final heave the structural financial deficit can be bridged for another year.
If that’s how the process goes, could any operational manager really implement these annual plans in real life? Not really. Then why is the annual contract so hard fought-over?
Quite simply because, every month (and I quote from the NHS Contract): “The amount to be paid shall be one twelfth of the individual Expected Annual Contract Value for the Commissioner.” These one-twelfth payments are the lifeblood of any Trust and are what pays the wage bill.
So I’m not particularly convinced that the annual planning process quite lives up to its promise.
There’s another problem, which is that it perpetuates planning as a series of once-off paper exercises, where really planning should be a continuous and live management process.
That’s not just a problem for the NHS, it’s also a problem for you as professionals. When something is seen more as a paper exercise than something real, with real consequences, that tends to lower the status of the people who do it, and make their role look less professional.
I think you can do something about that, and we’ll come back to it later on.
Short range operational planning
The other type of planning that is very common in the NHS is the kind of planning that operational managers do. This is where operational managers use their knowledge and experience of the current state of the services they run, to keep emergency work flowing over the coming days and achieve the 18 week targets at month-end.
The good thing about planning at such short range is that there’s a lot of certainty. They know from the PTL exactly which elective patients are coming up to breach and need booking in. And annual leave has been finalised so they know exactly which staff are on, and which beds and sessions are available.
If things are tight they can box and cox their way through: laying on extra sessions at short notice, moving patient appointments to stay under 18 weeks, finding capacity at the local private sector hospital, things that are bread and butter in a weekly operational meeting.
But the trouble is, all that short-range certainty isn’t a benefit at all. It’s a curse. Because it means that everything is pretty much set in stone. It’s actually really hard work to adjust capacity at such short range, precisely because annual leave is finalised, and because all the sessions have already been booked into.
Which is why it is so often referred to as fire-fighting.
When planning works well
You may have noticed that we just jumped all the way from planning the whole financial year, to planning the next couple of weeks, without having anything much in the middle. What I’m going to show you is how, by plugging that gap, we can fix lots of problems in one go.
How can we tell when planning is working well in the NHS? For me, the acid test has got to be that it changes real life for the better. If planning doesn’t change real life then quite frankly there is no point in doing it. And if it’s going to change real life, it has to be meaningful to clinicians and operational managers.
“Golden Zone”: the right time range
Getting the time range right is a good place to start.
As soon as you get more than 6 weeks into the future, operational managers have much more control over capacity. They can negotiate annual leave, open and close sessions because they haven’t been booked into yet, and generally adapt capacity all within the normal working week – instead of relying on ‘extra’.
What they lack (at the moment) is the information they need to make those judgements. Once you start giving managers planning information for this ‘golden zone’ that runs from 6 weeks to a few months into the future, it blows the fog away for them. Then they can turn your planning into reality.
And of course, any model that can cover that time range is also good for the longer-range plans too.
Up to date
One of the difficulties with annual planning is that it gets out of date. All you need is for a consultant to go off sick, or norovirus, or a bowel cancer awareness campaign, and all bets are off.
So if you keep your planning refreshed every month, or even every week, then your planning is topical and more likely to be acted upon. Put it another way: in this game, it’s more important to be adaptive than to be accurate.
Detailed
The NHS planning process traditionally runs at specialty level. But if you go to an operational manager with, say, an overall plan for orthopaedics, you may get a sceptical look because they know their problems are in joint replacements or spinal surgery. They aren’t so interested in an aggregate figure that has hands and feet bundled into the mix.
The ideal level of detail is the level of inflexibility: in orthopaedics that might be a split between upper limb, lower limb, and spines. Or it might be more detailed than that. It depends on how your clinical teams are organised, and operational managers can give you a steer on the best way to reflect this in the modelling. If some consultants straddle more than one subspecialty then there may be enough flexibility to keep things simple and lump them together.
So usually subspecialty is the level of detail you want to get to, and it’s good that the new system resilience plans are going that way. A typical PAS doesn’t have subspecialties coded in, but you can usually do it relatively easily by grouping consultants into subspecialties.
Week by week
In terms of detail it also pays to break the plan down week by week.
The annual planning round just models the whole year in one big lump, which tells operational managers what they have to do, but doesn’t give them any clue about how.
Breaking it down pro rata month by month, as financial plans tend to do, doesn’t help either because (as every analyst knows) months vary a lot by how many working days they have.
So you have to model in weeks: that’s the unit of time operational managers use, with sessions being organised on weekly, 2-weekly, and 4 or 5-weekly cycles; and everyone agrees how long a week is.
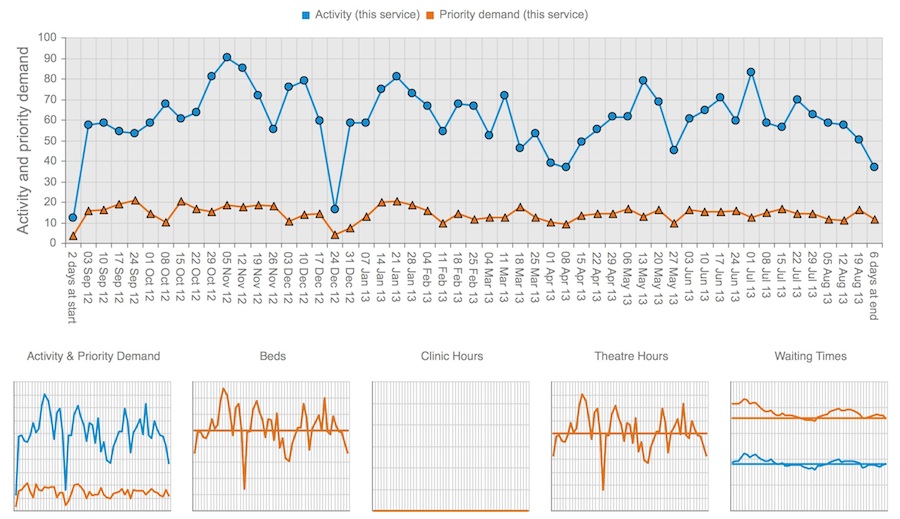
The screenshot above is taken from Gooroo Planner. Once you get down to weeks, you can suddenly see things like Christmas, Easter and the summer holidays all emerging in the patterns. And you can see how that pans out for activity, capacity, and waiting times.
That’s good, not just because it reflects real life, but because it gives operational managers the confidence that their plans relate to their experience.
Operationally owned
One of the things we touched on earlier is the importance of operational managers believing in the performance assumptions being used. It’s fair enough: they’re the ones who get it in the neck if it goes wrong. We’re talking about things like theatre utilisation, length of bed stay, clinical urgency rates, removal and cancellation rates, that kind of thing.
And this is where I think there is a big opportunity for analysts as a profession.
Because when planning is real, somebody needs to help operational managers model through the implications of different performance assumptions, understand how much they can help close any gaps, and plan exactly how elective activity can be reprofiled around the winter peak without blowing up waiting times.
Then, once operational managers know the performance and activity profiles they’re aiming for, somebody needs to gather all those assumptions into one place and curate them. So every time any kind of planning exercise is done, the right assumptions are used: the ones owned by the operational managers.
I think it’s fairly obvious that that somebody should be a professional analyst. And this is a big role.
Being the central curator of the organisation’s performance assumptions is not only a very central role, but it’s also very operationally engaged. I don’t think it really exists yet in most Trusts. But it should be an essential role with strong links to operations.
Professional
It should go without saying that good planning needs valid methods, but it is rather surprising what passes for planning sometimes.
For instance there is the sum that goes like this: I’ve got this many consultants, and they’ve got this many sessions each, and they treat this many patients per session; so if I multiply that up then that’s my plan.
Where is the demand for healthcare in that calculation? Nowhere.
Will they keep up with demand and achieve 18 weeks? There is no way of knowing.
That sum is alright as an estimate of capacity. But that shouldn’t necessarily be the plan. If plans are based on capacity, not demand, then waiting times are going to end up taking a long walk, who knows where.
So all planning has to start with demand.
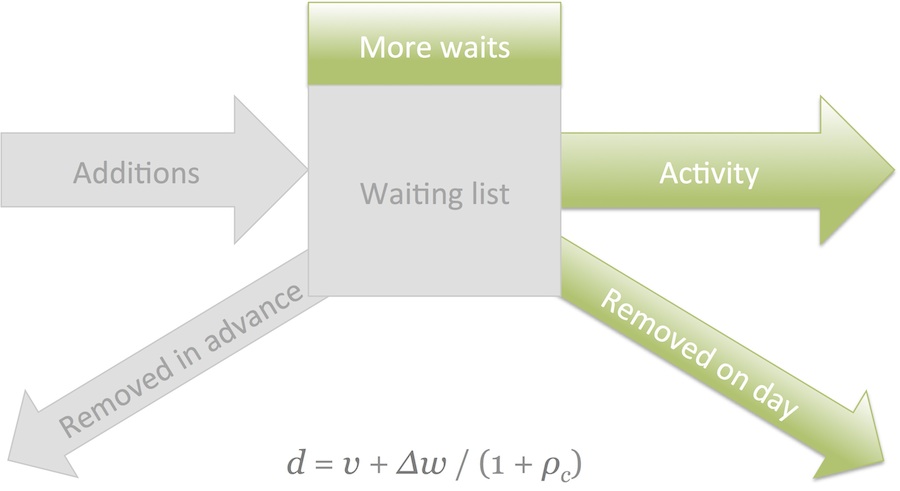
How do we measure demand? Emergency demand is pretty straightforward, because it’s the same as activity.
But calculating the demand for elective care is tricky, especially when the most obvious data to use is also the most error-prone: additions to the waiting list. But there are solutions in the maths, and one is shown above.
It also gets tricky a bit further down the patient pathway, when you want to split out the underlying and knock-on causes of inpatient and daycase demand. But again with a bit of care there are solutions to that too.
Then for those services that are covered by waiting times targets, your planning also needs to be based on a thorough understanding of waiting times dynamics, because waiting times are a function of both the size of the waiting list and the way it’s being managed. That includes the impact of clinical urgency, removals, and good patient scheduling tactics.
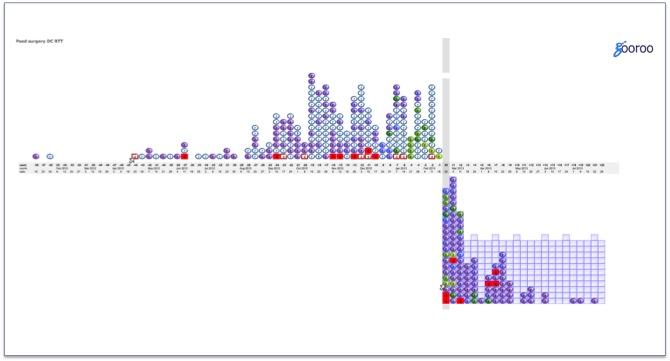
This is a screenshot from Gooroo SimActive, of a real NHS waiting list. In ten minutes I could teach you how to use this analysis to identify not just long waiting times but also: clinical risk to patients, poor patient scheduling, poor capacity utilisation, and poor resource allocation… and to show how all those things can be improved within current resources, and to create an environment so that consultants can initiate all those changes themselves.
So for professional modelling you should start from demand, have a good understanding of waiting times dynamics, and most of the rest is accepted methodology.
Automated
If all your planning is going to be done properly like this, we’re looking at quite a lot of numbers.
Let’s say your Trust has 60 subspecialties; each split 5 ways for the various stages of treatment; for 52 weeks of the year; with say 180 input data items and the same again in results items: that’s a planning model of over 100,000 data points.
When you’re refreshing it monthly or perhaps weekly, I hope you’ll agree we are some way beyond the usefulness of Microsoft Excel. The risk of cut and paste errors alone is going to cause trouble.
That’s why, when we set about building Gooroo Planner, we decided to go for the industrial strength solutions by developing purpose-built software, powered by a big database, running on a beefy server, and with an API to allow automation.
With that kind of technology you can run huge models in a matter of seconds, and keep your plans automatically refreshed without any human intervention.
Distributed
The automation is all very whizzy, but really it is the distribution technology that makes the biggest difference. You need to deliver your planning to the people who are going to rely on it: operational managers and clinicians.
Some of you already use reporting software like Tableau or QlikView to deliver self-service performance monitoring throughout your organisations. Others of you are still emailing spreadsheets around, or putting them on shared drives.
However you do it, you need to distribute your planning through the same medium that you already distribute your performance monitoring. You don’t want people to have to visit several different services to get their information.
So when operational managers look up their outturn activity or size of waiting list, they can see their plans automatically overlaid on the same chart. Like this.
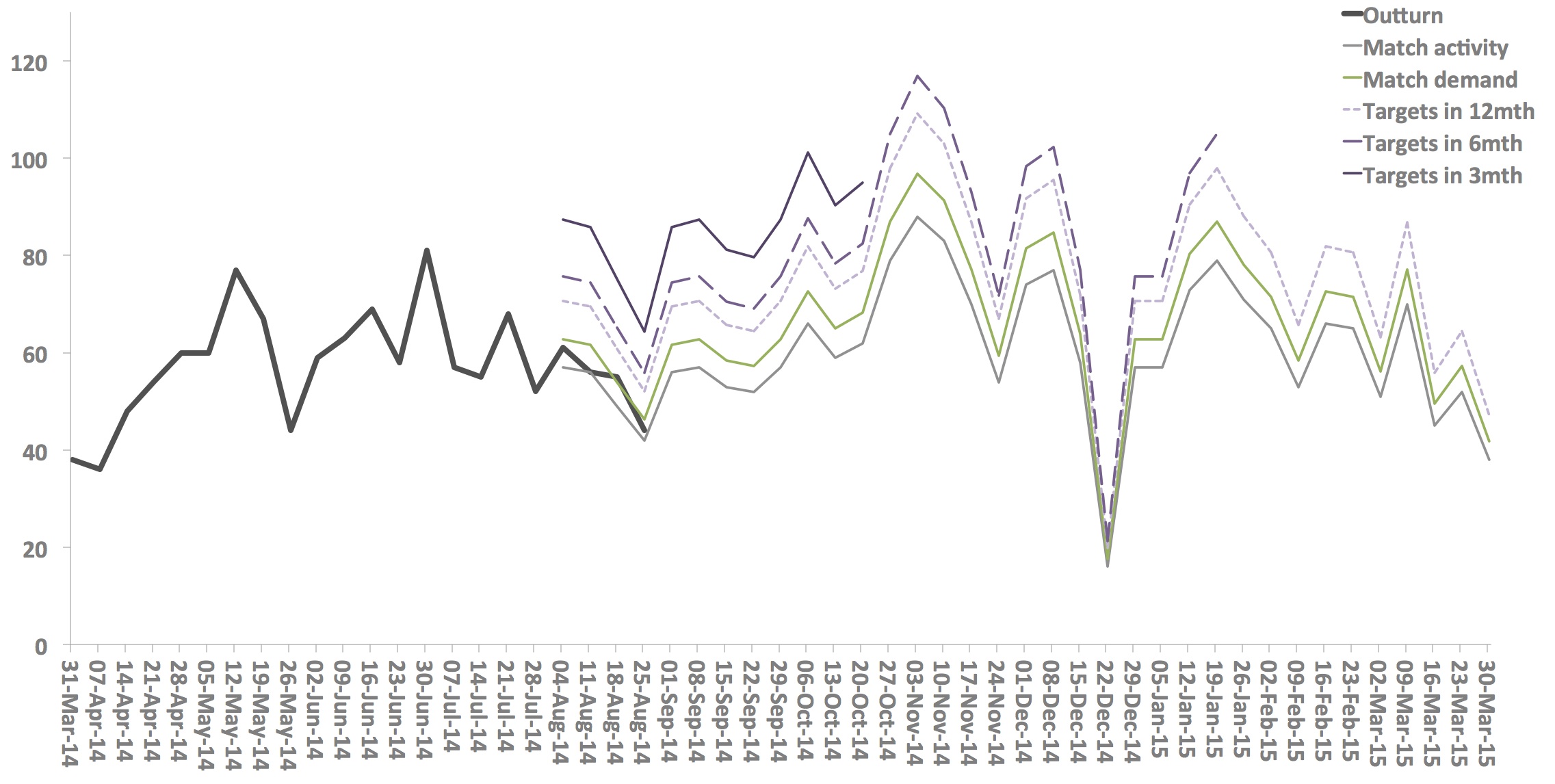
Not just one plan either, but probably a series of plans, ranging from business as usual, through keeping up with demand, to achieving all targets in 12 months or 6 months or 3 months.
Then if their outturn is falling short of what is needed, they can see which trajectory they are closest to. In the mockup above you can see that they are just about keeping up with demand, but will never achieve their targets.
Conclusion
We’ve seen how you can deliver planning that covers the ‘golden zone’ from 6 weeks to a few months ahead, is always up-to-date, detailed and comprehensive, rich in week-by-week detail, owned by operational managers, professional and demand led, refreshed automatically while you sleep, and distributed throughout the organisation.
Because the assumptions and activity profiles must be genuinely owned and driven by operational managers, there is a vital and largely new role for professional analysts: to model the impact of those scenarios with operational managers, to help operational managers decide what they want to do, and to be central curators of every operational division’s performance assumptions for the whole organisation.
The title of my talk is “Capacity planning: feed-the-beast, or vital management information?” It’s a rhetorical question of course. It should and must be vital management information.
The difference now is that network and database technologies have finally made it possible.
Return to Post Index
Leave a Reply
You must be logged in to post a comment.